The New York City Council Committee on Health, Committee on Hospitals, and Committee on Women and Gender Equity held an oversight hearing on maternal mortality and morbidity in New York City on December 7, 2020. NYHealth submitted written testimony on the status of maternal health in the City.
December 9, 2020
Distinguished Members of the Committee on Health, Committee on Hospitals, and Committee on Women and Gender Equity:
The New York Health Foundation (NYHealth) appreciates the opportunity to submit written testimony on the status of maternal health in New York City. We offer information from our recent research report on severe maternal morbidity in New York to add to the evidence base of racial and ethnic disparities in maternal health outcomes. In addition, we identify policy approaches for consideration to support and encourage the use of midwives and community-based health workers to reduce incidence of severe maternal morbidity, close disparities by race and ethnicity, and accommodate patient choice.
The Status of Maternal Health in New York City
The United States has a higher maternal mortality rate compared to other peer developed nations.1, 2 Unfortunately, maternal death is considered the “tip of the iceberg” of an even larger body of adverse maternal events impacting women.3, 4 Prior research has found that for every maternal death, there are up to 100 occurrences of severe maternal morbidity (SMM).5 SMM refers to outcomes during labor and delivery that result in adverse short- or long-term consequences to a woman’s health.6 These outcomes may be life-threatening and require the need for lifesaving procedures, such as a blood transfusion or ventilation.7
New York State has historically had higher rates of SMM than the rest of the nation. The most recent years of nationwide data show that New York State ranked in highest quartile of state SMM rates.8 Prior research has documented the high rates of SMM and racial and ethnic disparities in New York City specifically. 9, 10,11 This is particularly concerning given that, in 2018, New York City accounted for approximately half (49%) of all deliveries in the State, including more than half of all Black and Hispanic deliveries. There are significant disparities in SMM by race and ethnicity in New York City, even after controlling for differences in health status, insurance type, sociodemographic characteristics, education, prenatal care, and socioeconomic status.12, 13
NYHealth’s Work to Improve Maternal Health
NYHealth is a private, independent foundation that works to improve the health of all New Yorkers, especially the most vulnerable. Our grantmaking and research has provided us with experience in and knowledge of the disparities in maternal health across New York State. In particular, through our Empowering Health Care Consumers program, we have supported work to expand access to transparent information about maternal health care quality and outcomes.14
NYHealth has recently funded multiple projects to enable New Yorkers to make informed and higher-value decisions about maternity care. This includes the development of an online tool that allows expectant mothers to compare local providers in the New York City area based on quality measures and other factors that affect maternity and newborn care.15 In addition, the Foundation is supporting an effort by one of the largest unions in the State to develop a high-value maternity care network for its expectant parents, who are predominantly lower-wage union workers and women of color.16, 17
New Research on Severe Maternal Morbidity in New York City
At this critical juncture, NYHealth would like to provide the Committees with new research that sheds light on the stark racial and ethnic disparities in severe maternal morbidity in New York City. This analysis can support the City in its continued efforts to design programs and target resources. Below are key findings from a 2020 NYHealth analysis of SMM, using 2011–2018 inpatient hospital admissions associated with deliveries.
- 3,311 deliveries in New York City in 2018 were associated with an SMM event, out of the 102,268 inpatient hospital admissions associated with deliveries analyzed.18 This translates to an overall SMM rate of approximately 324 out of every 10,000 deliveries (or 3.2%) (see Figure 1). This was higher than the overall New York State rate (2.7 %).
- In 2018, New York City had the highest rate of SMM in the State, with an SMM rate more than three-and-a-half times larger than the region with the lowest rate (324 per 10,000 deliveries in New York City, compared to 90 per 10,000 in the Finger Lakes) (see Figure 2).
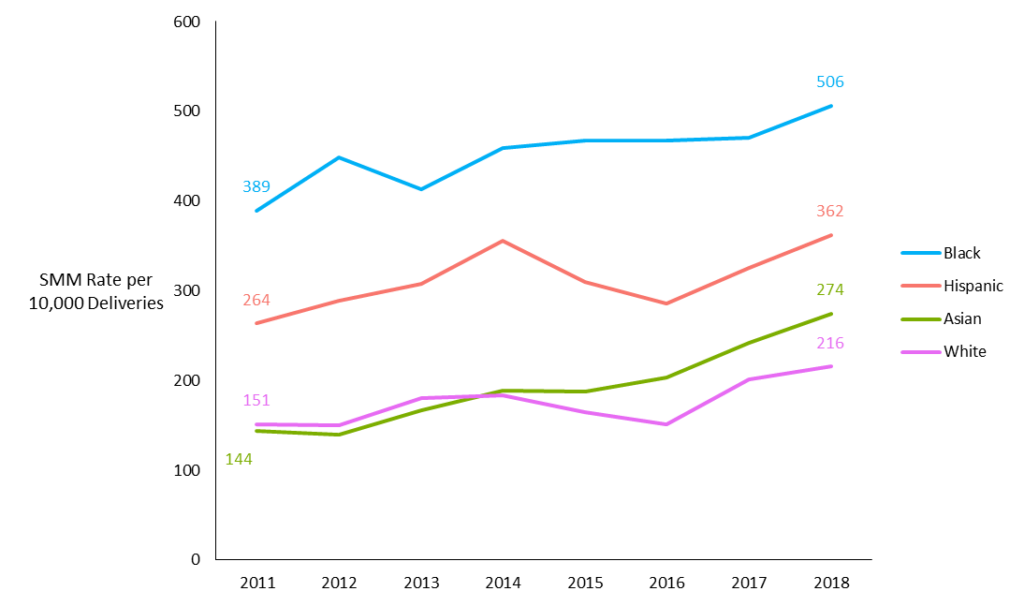
- Disparities in SMM by race and ethnicity persisted in New York City from 2011 through 2018 (see Figure 3). In 2018, the SMM rate for Black women was 506 per 10,000 deliveries, amounting to 2.3x the rate for white women.19 The rate for Hispanic women was approximately 1.7x the rate for white women; the rate for Asian women was approximately 1.3x the rate for white women (362 and 274 per 10,000, respectively, compared to 216 per 10,000). For Black and Hispanic women, these are similar disparities as in 2011 (2.6x for Black women and 1.7x for Hispanic women).
- Racial and ethnic disparities were present both for populations covered by Medicaid and those covered by private insurance plans. Substantial racial and ethnic disparities were also present across both vaginal and cesarean deliveries.
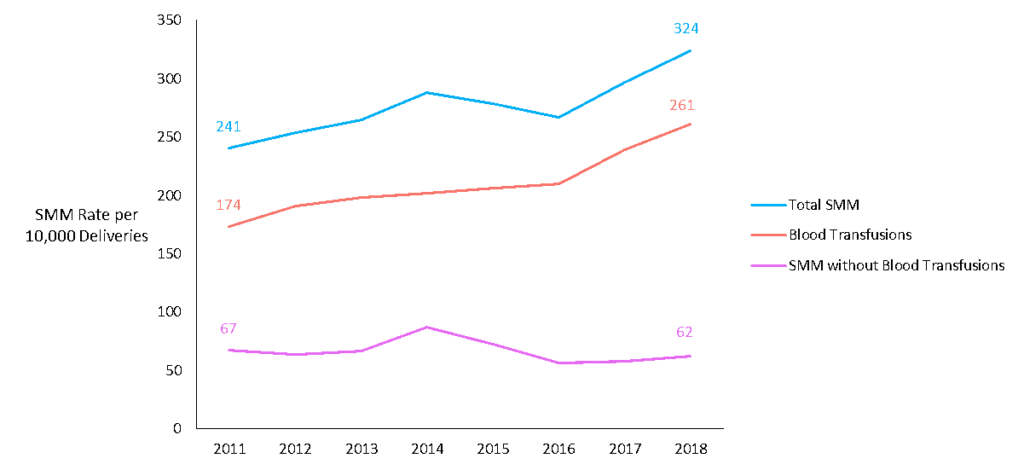
- The majority of SMM events were related to blood transfusions (see Figure 4). Blood transfusions are a proxy for identifying hemorrhage, a form of SMM, but can be an imperfect indicator of SMM. The recent increase in blood transfusion may reflect increased quality improvement efforts in New York to mitigate maternal hemorrhage. However, there remain racial and ethnic disparities in SMM cases with and without blood transfusions.
For more details about this data, please see our full report, available here: https://nyhealthfoundation.org/wp-content/uploads/2020/08/severe-maternal-morbidity.pdf.
Expanding the Role of Midwives and Community-Based Health Workers
Several important provisions have been implemented to reduce SMM and address racial and ethnic disparities in recent years at both the City and State levels. Our full report discusses recent efforts to increase quality improvement, improve data collection and monitoring, combat implicit bias, and facilitate access to community-based health workers. Recognizing that some of the causes of SMM, such as implicit racial bias, have been ingrained into the societal and health care system culture for decades, solutions must draw from all these domains and work in tandem. For example, while the City’s Maternal Mortality and Morbidity Review Committee identifies clinical trends by conducting case reviews of every maternal death in the City, the City’s Maternal Hospital Quality Improvement Network can use these data to provide hospital-specific recommendations to reduce disparities in preventable SMM. A coordinated, sustained, and aggressive effort will be required to permanently reduce SMM in New York City.
Joint planning between the City and State is vital to complement efforts, build upon models that work, and avoid duplication. For example, City involvement will be valuable to the State’s development of a data warehouse measuring hospital performance on perinatal quality measures.20 The State’s Perinatal Quality Collaborative is also currently developing an implicit racial bias curriculum for hospitals, which could build upon existing trainings conducted at NYC Health + Hospitals.21
Below, we provide input on the importance of midwives and community-based health workers in reducing incidence of SMM as one critical component of a multi-pronged solution. We then highlight key actions taken by the City and State to improve access to these services and advocate for these programs to be expanded and studied. Finally, we propose a bundled payment model as another pathway to increase access to midwifery and community-based health worker services at NYC Health + Hospitals.
The Benefit of Midwives and Community-Based Health Workers
Midwives and community-based health workers such as birth doulas and community health workers (CHWs) have been shown to play an important role in improving maternal health outcomes.22,23,24 From 2013–2017, the Center for Medicare & Medicaid Innovation developed and tested delivery models that integrate these health workers as part of the “Strong Start for Mothers and Newborns Initiative.”25 These models, which included a birth center model and a maternity care home model, had either equal or better outcomes than control models for the same or lower cost. The birth center model, led by midwives, was most consistently shown to result in comparatively better outcomes and lower costs.
Women of color may particularly benefit from midwifery and community-based health worker services. Research documents that women of color often experience disrespect—including racism and discrimination—during their pregnancy care, feel uninvolved in the clinical decision-making process, or do not feel that they have a voice in the delivery room.26 In addition to contributing to low-quality care, these events can increase the risk of SMM. Doulas and CHWs can help advocate for respectful care at the time of birth and by educating women about their rights during pregnancy. Providing access to midwifery services is also critical for respecting patient choice and reproductive autonomy.
Strategies to Increase Access to Midwives and Community-Based Health Workers
NYHealth applauds the City for facilitating access to doula services through its Healthy Women, Healthy Futures doula initiative, which has provided culturally-appropriate doula support to more than 1,000 clients as of 2019.27 The By My Side Birth Support Program (BMS), part of the federally-funded program Healthy Start Brooklyn, also offers free doula services to Medicaid-eligible clients in Brownsville and East New York.28 Importantly, BMS also sponsors doula trainings to increase the size and diversity of the City’s doula workforce. These programs are an important step toward guaranteeing access to doula care for all New Yorkers who want support in their pregnancy. However, the need for doula services is far greater than the capacity of these two programs and is not limited to the income groups and geographic areas currently served. The City should expand the capacity of these programs to serve more New Yorkers in all neighborhoods of New York City. The City should also consider supporting long-term assessments of these programs to provide evidence of the need for and effectiveness of such services.
The City should also build upon recent State initiatives to increase access to doulas and CHWs. The State launched a pilot program in 2019 to allow Medicaid reimbursement for doula services.29 The pilot program is currently operating in Erie County and was scheduled to launch in Kings County, but has failed to recruit an adequate number of doulas because of low reimbursement rates.30 Furthermore, the pilot excludes three ZIP codes in Brownsville and East New York, despite these areas having among the highest rates of poor birth outcomes in the City.31 Consideration should be given to adapt the Medicaid pilot to better support access to doulas in New York City, including expanding the program to areas with the highest rates of SMM, as well as paying an adequate amount for doula services.
The State also funds the Department of Health’s Maternal Infant Community Health Collaboratives (MICHC) to increase access to CHWs.32 In New York City, six MICHC projects are collaborating with community partners and health workers to engage high-need women in health care and social services.33 CHWs have played an important role during the COVID-19 pandemic in New York, working with pregnant women remotely to navigate the rapidly changing environment of maternity care and hospital delivery. For example, Public Health Solutions (PHS), which operates the Queens MICHC project, innovatively adapted its community health worker model in response to COVID-19 to continue supporting expectant and new parents via phone and video visit.34 The City should build upon these existing CHW projects and consider conducting assessments to better understand how to maximize the effectiveness of such services.
Finally, the City should consider innovative payment models as a pathway to increase access to midwife, doula, and CHW services at the City’s public hospital system. One such model is a bundled payment model for deliveries. In a bundled payment model, a payer pays a lump sum for all medical care associated with pregnancy. A bundled payment model supports a more holistic and coordinated approach to care, as one payment could cover the entire prenatal period, labor and delivery, and the postpartum time period for both mother and newborn. Providers are incentivized to work together and use higher-value and evidence-based models—such as those that use birth centers, midwives, CHWs and doulas—in order to manage costs below the lump sum. In this way, a bundled payment model for maternity care accommodates patient choice, as the health system would be better positioned to receive reimbursement for a wider variety of care models that can meet the unique preferences, beliefs, and needs of their patients.
Several commercial payers and state Medicaid programs are beginning to test bundled payment models for maternity care across the country.35,36 ,37 Such models have also been widely tested for other types of services (e.g., hip and knee replacements), resulting in lower, more predictable costs, as well as higher quality care.38 The City Council should consider how to use its oversight role over the NYC Health + Hospitals public health care system to encourage and support the use of bundled payment models. NYC Health + Hospitals accounts for a substantial proportion of births in the City, particularly in lower-income areas at higher risk for SMM. Matching the payment model with new, innovative delivery system models is critical to help ensure improved access to midwife, doula, and CHW services that can accommodate birthing choice and improve health outcomes.
Conclusion
NYHealth is grateful for the shared commitment among stakeholders to improve maternal health in New York City and close racial and ethnic disparities. While there is no one solution to combat SMM, a sustained and multi-pronged effort—one that includes expanded access to midwives and community-based health workers—will help improve health outcomes for pregnant New Yorkers. We look forward to continuing our partnerships with the City and other organizations to achieve this goal.
Appendix
Fig 1. Severe Maternal Morbidity Rates in New York City: 2011–2018
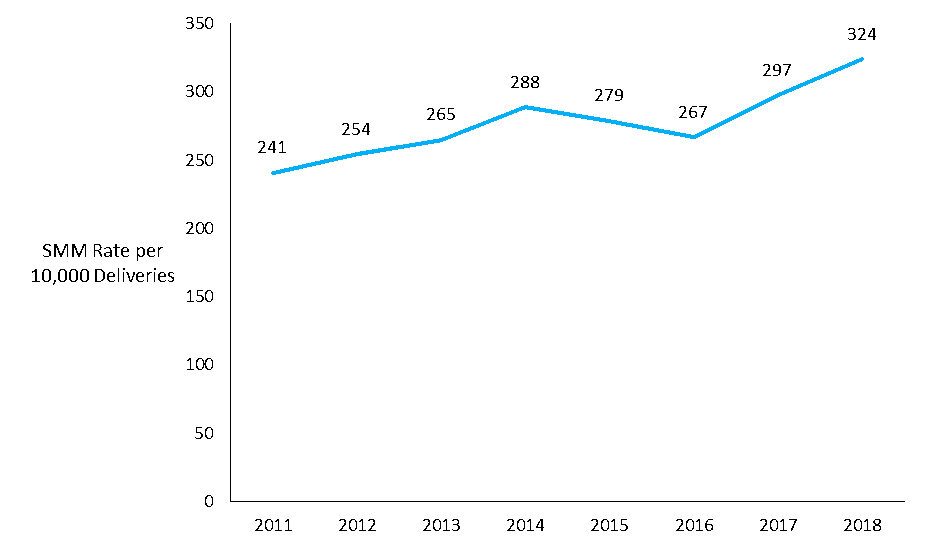 Source: New York Health Foundation analysis of 2011–2018 New York State Statewide Planning and Research Cooperative System (SPARCS) data.
Source: New York Health Foundation analysis of 2011–2018 New York State Statewide Planning and Research Cooperative System (SPARCS) data.
Notes: See full report for details on the data and SMM rate calculation, including the number of deliveries in total.
Fig 2. Severe Maternal Morbidity Rates by Region of New York State: 2018
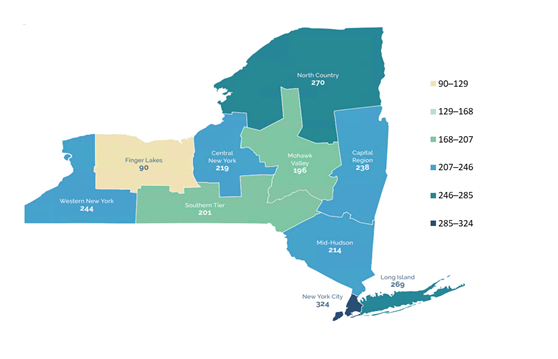
Source: New York Health Foundation analysis of 2011–2018 New York State Statewide Planning and Research Cooperative System (SPARCS) data.
Notes: See full report for details on the data and SMM rate calculation, including the total number of deliveries by region used in the analysis. New York’s Empire State Development Corporation regions are used to identify regions: https://esd.ny.gov/regions.
Fig 3. Severe Maternal Morbidity Rates by Race and Ethnicity in New York City: 2011–2018
Source: New York Health Foundation analysis of 2011–2018 New York State Statewide Planning and Research Cooperative System (SPARCS) data.
Notes: Non-Hispanic Black women are categorized as Black, non-Hispanic Asian women are categorized as Asian, and non-Hispanic white women as categorized as white. See full report for details on the data and SMM rate calculation.
Fig 4. Severe Maternal Morbidity Rates with and without Blood Transfusions in New York City: 2011–2018
Source: New York Health Foundation analysis of 2011–2018 New York State Statewide Planning and Research Cooperative System (SPARCS) data.
Notes: See full report for details on the data and SMM rate calculation. In this figure, the “SMM with Blood Transfusions” line includes deliveries where a blood transfusion was the only indicator of SMM, and deliveries where a blood transfusion was an indicator along with another, non-blood transfusion indicator of SMM.
[1] World Health Organization, “Trends in Maternal Mortality 2000 to 2017: Estimates by WHO, UNICEF, UNFPA, World Bank Group and the United Nations Population Division,” 2019, https://www.who.int/reproductivehealth/publications/maternal-mortality-2000-2017/en.
[2] Munira Gunja et al., “What Is the Status of Women’s Health and Health Care in the U.S. Compared to Ten Other Countries?” (The Commonwealth Fund, December 2018), https://www.commonwealthfund.org/publications/issue-briefs/2018/dec/womens-health-us-compared-ten-other-countries.
[3] It is important to note that not all people facing these issues identify as women.
[4] William M. Callaghan, Andreea A. Creanga, and Elena V. Kuklina, “Severe Maternal Morbidity among Delivery and Postpartum Hospitalizations in the United States,” Obstetrics and Gynecology 120, no. 5 (November 2012): 1029–36, https://doi.org/10.1097/aog.0b013e31826d60c5.
[5] Callaghan, Creanga, and Kuklina.
[6] Centers for Disease Control and Prevention, “Severe Maternal Morbidity in the United States,” January 31, 2020, https://www.cdc.gov/reproductivehealth/maternalinfanthealth/severematernalmorbidity.html.
[7] American College of Obstetricians and Gynecologists and the Society for Maternal–Fetal Medicine, Sarah K. Kilpatrick, and Jeffrey L. Ecker, “Severe Maternal Morbidity: Screening and Review,” American Journal of Obstetrics and Gynecology 215, no. 3 (2016): B17-22, https://doi.org/10.1016/j.ajog.2016.07.050.
[8] See attachment “ALL FAD – June 8 2020.xlsx” contained within: HRSA Maternal and Child Health, “Federally Available Data” (U.S. Department of Health and Human Services, July 2, 2020), https://mchb.tvisdata.hrsa.gov/uploadedfiles/TvisWebReports/Documents/FADResourceDocument.pdf.
[9] New York City Department of Health and Mental Hygiene, “Severe Maternal Morbidity Surveillance,” July 3, 2018, https://www1.nyc.gov/assets/doh/downloads/pdf/data/severe-maternal-morbidity-data.pdf.
[10] Elizabeth A. Howell et al., “Site of Delivery Contribution to Black-White Severe Maternal Morbidity Disparity,” American Journal of Obstetrics and Gynecology 215, no. 2 (2016): 143–52, https://doi.org/10.1016/j.ajog.2016.05.007.
[11] Elizabeth A. Howell et al., “Race and Ethnicity, Medical Insurance, and Within-Hospital Severe Maternal Morbidity Disparities,” Obstetrics and Gynecology 135, no. 2 (2020): 285–93, https://doi.org/10.1097/AOG.0000000000003667.
[12] Howell et al., “Site of Delivery Contribution to Black-White Severe Maternal Morbidity Disparity.”
[13] Howell et al., “Race and Ethnicity, Medical Insurance, and Within-Hospital Severe Maternal Morbidity Disparities.”
[14] New York Health Foundation, “Empowering Health Care Consumers,” accessed December 1, 2020, https://nyhealthfoundation.org/what-we-fund/empowering-health-care-consumers/.
[15] ExpectNY, “Information That Empowers,” accessed December 1, 2020, https://expectny.com.
[16] “Building Service 32BJ Health Fund,” New York Health Foundation, accessed December 1, 2020, https://nyhealthfoundation.org/grantee/building-service-32bj-health-fund/.
[17] Melanie Grayce West, “New York City Union Uses Its Size to Leverage Improved Maternity Care,” The Wall Street Journal, August 19, 2019, https://www.wsj.com/articles/new-york-city-union-uses-its-size-to-leverage-improved-maternity-care-11566256083.
[18] SMM is identified using a definition developed by the Centers for Disease Control and Prevention. See: Centers for Disease Control and Prevention, “How Does CDC Identify Severe Maternal Morbidity?,” December 26, 2019, https://www.cdc.gov/reproductivehealth/maternalinfanthealth/smm/severe-morbidity-ICD.htm.
[19] In this report, we categorize non-Hispanic Black women as Black, non-Hispanic Asian women as Asian, and non-Hispanic white women as white.
[20] State of New York Office of the Budget, “Governor Andrew Cuomo Announces Highlights of the FY 2020 State Budget,” April 1, 2019, https://www.budget.ny.gov/pubs/press/2019/pr-enactfy20.html.
[21] State of New York Office of the Budget.
[22] Vivienne Souter et al., “Comparison of Midwifery and Obstetric Care in Low-Risk Hospital Births,” Obstetrics and Gynecology 134, no. 5 (2019): 1056–65, https://doi.org/10.1097/AOG.0000000000003521.
[23] Kenneth J. Gruber, Susan H. Cupito, and Christina F. Dobson, “Impact of Doulas on Healthy Birth Outcomes,” The Journal of Perinatal Education 22, no. 1 (2013): 49–58, https://doi.org/10.1891/1058-1243.22.1.49.
[24] Centers for Disease Control and Prevention, “Policy Evidence Assessment Report: Community Health Worker Policy Components” (Atlanta, GA: Centers for Disease Control and Prevention, 2014), https://www.cdc.gov/dhdsp/pubs/docs/chw_evidence_assessment_report.pdf.
[25] Centers for Medicare and Medicaid Services, “Strong Start for Mothers and Newborns Initiative: Enhanced Prenatal Care Models,” July 28, 2020, https://innovation.cms.gov/innovation-models/strong-start-strategy-2.
[26] Monica R. McLemore et al., “Health Care Experiences of Pregnant, Birthing and Postnatal Women of Color at Risk for Preterm Birth,” Social Science & Medicine 201 (2018): 127–35, https://doi.org/10.1016/j.socscimed.2018.02.013.
[27] New York City Department of Health and Mental Hygiene, “The State of Doula Care in NYC 2019,” 2019, https://www1.nyc.gov/assets/doh/downloads/pdf/csi/doula-report-2019.pdf.
[28] New York City Department of Health and Mental Hygiene.
[29] New York State Department of Health, “New York State Doula Pilot Program,” November 2020, https://www.health.ny.gov/health_care/medicaid/redesign/doulapilot/index.htm.
[30] New York City Department of Health and Mental Hygiene, “The State of Doula Care in NYC 2019,” accessed December 2020, https://www1.nyc.gov/assets/doh/downloads/pdf/csi/doula-report-2019.pdf.
[31] New York City Department of Health and Mental Hygiene.
[32] State of New York Office of the Budget, “Governor Andrew Cuomo Announces Highlights of the FY 2020 State Budget.”
[33] New York State Department of Health, “Maternal and Infant Community Health Collaboratives Initiative,” October 2020, https://www.health.ny.gov/community/adults/women/maternal_and_infant_comm_health_collaboratives.htm.
[34] Public Health Solutions, “Supporting Expectant and New Parents during COVID-19,” https://nyhealthfoundation.org/event-recap/practically-speaking-supporting-expectant-and-new-parents-during-covid-19/.
[35] Clare Pierce-Wrobel and Katie Green, “To Help Fix The Maternal Health Crisis, Look To Value-Based Payment,” Health Affairs Blog (blog), July 16, 2019, https://www.healthaffairs.org/do/10.1377/hblog20190711.816632/full/.
[36] Carmen Heredia Rodriguez, “Insurers Test New Way To Cut Maternity Care Costs: Bundling,” Kaiser Health News, September 27, 2019, https://khn.org/news/maternity-care-bundling-payments-insurance-cesarean-sections/.
[37] Elizabeth Whitman, “Bundles of Joy? How New Payment Models for Maternal Care Could Deliver Lower Costs,” Modern Healthcare, April 13, 2016, https://www.modernhealthcare.com/article/20160813/MAGAZINE/308139965/bundles-of-joy-how-new-payment-models-for-maternal-care-could-deliver-lower-costs.
[38] Centers for Medicare and Medicaid Services, “Comprehensive Care for Joint Replacement Model,” November 24, 2020, https://innovation.cms.gov/innovation-models/cjr.
